Usted está aquí
Peruvian Journal of Neurosurgery
Awake Craniotomy for resection of low grade glioma. First experience in Perú 2008
Jerson Flores C.MD, Betty Quintanilla C.MD, Alejandro Rosell O.MD, Flor Arrese M. MD
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
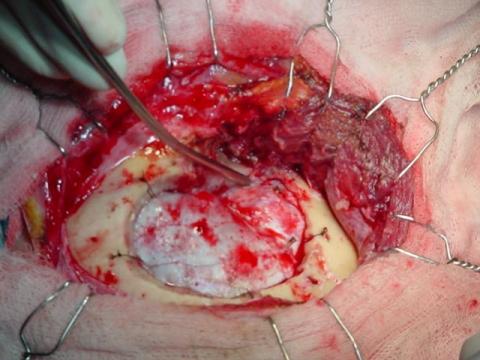
The aim of the brain tumour surgery is the maximal tumour resection with the minor neurological post operatory deficit; nevertheless this is not always possible mainly in case of lesions near to functional areas. Despite the use of numerous technologies of images before and during and during the operative period, the functional result is unknown but after the surgery when the deficit is irreversible. The awake craniotomy is a safe technique and that it allows to evaluate the neurological status during the surgical act and to detect prematurely any deficit in the function, which allow us optimize the results of the tumour resection. We presented the first report of case in Peru of awake craniotomy for low grade glioma resection, carried out in the Guillermo Almenara National Hospital in February 2008.
Key Words: Awake Craniotomy, surgery, low grade astrocytoma

Technique of the “cono embossed or cone of cookie” on the reconstruction of the neck at displastic giant aneurysm of the carotide paraoftalmic siphon: Intra-aneurismal Stent
Ricardo Vallejos T., Johan Choque V.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
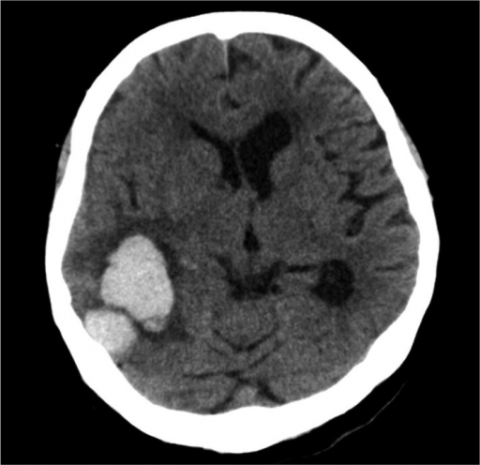
The dysplastic giant aneurysm with wide neck is a difficult complex aneurysm surgery, the use of endovascular therapy in this pathology is promising and waffle cone technique is very useful in those in wich when we use a Stent and it is impossible to exceed the distal end of the aneurysm neck. A woman patient of 73y, housewife with disease duration of 5 days, headache associated with neck stiffness and cranial nerve VI paresis of the left was studied. The brain CT showed subarachnoid hemorrhage in the left sylvian valley and an image suggestive of a giant aneurysm of left carotid siphon. The angiographic study concluded giant-ophthalmic aneurysm ruptured left and right paraoftálmic large aneurysm not broken.
The treatment of choice for aneurismal disease is still under discussion, but in the case of giant aneurysm endovascular techniques may achieve optimal results without major complications, endovascular technique waffle cone through the use of Stents is very useful and should extend its use in those dysplastic giant aneurysm with wide neck do not allow the stent to achieve beyond the distal aneurismal neck and both nest in the pouch is able to embed a Neuroform Stent-in the neck of the aneurysm to proceed to use coils of different dimensions to completely embolize the aneurysm. The disadvantages of this technique are the potential for drilling and higher rate of recanalization caused by changes in arterial blood flow. Waffle cone technique is particularly useful in those dysplastic giant aneurysms with wide neck in wich the structure of the aneurysm does not allow the location of the stent at the distal end of its neck.
Key words: Giant intracranial aneurysm, embolization, stents, subarachnoid hemorrhage.

Subarachnoid hemorrhage II: Cerebral aneurysms
Alberto Trelles P.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Subarachnoid hemorrhage (SAH) is defined as the presence of blood in the subarachnoid space and cisterns of the base. The source is variable and may be due to rupture of intracranial aneurysms (80%), arteriovenous malformations (AVMs), tumors and trauma cranoencefálicos. The HSA is a relatively common disease with an incidence is 5% of cerebral vascular disease. The estimated prevalence of 10 new cases per 100,000 people each year. The proportion of HSA varies with age, being the most prevalent group between 50 and 60. It is a pathology with high morbidity and mortality, since a high percentage of patients (10-15%) did not reach the hospital and the remaining group of about 15% die. Angiography is the standard diagnostic procedure, although angiography is an important alternative. Treatment should be administered as soon as possible within 72 hours, both surgical and endovascular techniques to prevent complications such as rebleeding, vasospasm and hydrocephalus, being the most widely used surgical approach is the pterional craniotomy. The prognosis depends on careful handling and the degree of the initial hemorrhage.
Key words: Subarachnoid hemorrhage, Intracraneal aneurysm, Craniotomy.

Subarachnoid hemorrhage I: Diagnosis and Management
Alberto Trelles P.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Subarachnoid hemorrhage (SAH) is defined as the presence of blood in the subarachnoid space and cisterns of the base. The source is variable and may be due to rupture of intracranial aneurysms (80%), arteriovenous malformations (AVMs), tumors and trauma cranoencefálicos. The HSA is a relatively common disease with an incidence is 5% of cerebral vascular disease. The estimated prevalence of 10 new cases per 100,000 people each year. The proportion of HSA varies with age, being the most prevalent group between 50 and 60. It is a pathology with high morbidity and mortality, since a high percentage of patients (10-15%) did not reach the hospital and the remaining group of about 15% die. Angiography is the standard diagnostic procedure, although angiography is an important alternative. Treatment should be administered as soon as possible within 72 hours, both surgical and endovascular techniques to prevent complications such as rebleeding, vasospasm and hydrocephalus, being the most widely used surgical approach is the pterional craniotomy. The prognosis depends on careful handling and the degree of the initial hemorrhage.
Key words: Subarachnoid hemorrhage, Intracraneal aneurysm, Craniotomy.
Pterional Keyhole Approach for treatment of Aneurysms 2009
Jerson Flores C., Alfredo Fuentes-Dávila M., Wesley Alaba G.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Objective: The pterional approach is the most common approach in vascular neurosurgery, but in recent years has been an increasing interest in minimally invasive surgery or keyhole surgery. We present preliminary results from the use of pterional keyhole approach in surgery for cerebral aneurysms performed in the Cayetano Heredia Hospital in 2009.
Patients and Methods: We performed a pterional keyhole craniotomy of 2.5 x 3 cm from a curved incision of approximately 5-6 cm behind the hairline and centered on the orbitofrontal and posterior aneurysm clipping, in patients with late aneurysms, CoP, bifurcation ICA and MCA aneurysms, Hunt and Hess I-III, without edema, associated vasospasm or hematoma.
Results: From January to December 2009 six patients were operated by pterional keyhole approach, 4 with CoP aneurysms (66%), 1 with ACI (17%) and 1 with ACM (17%). All were operated on late and Hunt and Hess was I in 3 cases (50%) III in 2 cases (33%) and II (17%). There were no operative complications and the outcome was favorable in most cases: Rankin 1 (50%) and Rankin 2 (33%).
Conclusions: The pterional keyhole approach is a minimally invasive surgery for brain aneurysms, which maintains the advantages of the standard pterional approach but it minimizes the exposure of brain parenchyma and soft tissue manipulation. It is a valid surgical alternative in selected cases, mainly from CoP and MCA aneurysms.
Key Words: Pterional approach, craniotomy, aneurysms, minimally invasive.
Two years of Lumbo-sacral spine dynamic stabilization in Rebagliati-Essalud Hospital during the period January 2012-October 2013
Miguel Vizcarra F., José Navarro B., Carlos Suárez M., Arturo Morales D.,
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Objective: To determine the clinical outcome in patients undergoing dynamic stabilization in the neurosurgery spine service at HNERM during the period January 2012 to October 2013.
Methods: 25 patients with unstable spine that met the inclusion criteria for the placement of dynamic spine stabilization were selected.
Results: The average age of patients 46.4 years, minimum 6 and maximum 78 years. Sex: Male 16 (64%) Female 09 (36%) total 25 (100%). No previous lumbar 23 (92%), discectomy 02 (08%): prior lumbar surgery Sick time (months) 25.8 average, minimum 3 and maximum 72. Surgical approach Wiltse Total 15 (60%), medial approach 9 (36%) type, Hoober 1 (4%) 25 Instrumentation levels; 2 level 4 (16%), three levels 21 (84%). Days in hospital: average 3.72 min 3 max 5. Preoperative clinical features: EVA average 7.92 min 6 max 10 mod 8. Pain intensity mod 13 (52%), severe12 (48%). Postoperative clinical features: EVA average 4.16 min 3 max 8 fashion: 3. Pain intensity: mild 19 (76%), moderate 05 (20%) and severe 04 (14%).
Conclusions: Dynamic stabilization has demonstrated efficacy in pain control with a minimum length of hospitalization.
Key words: lumbosacral unstability , dynamic stabilization, pain control effectiveness

Transoral decompression and posterior fixation in atlanto – axial instability
Alfredo Fuentes Dávila M. , Wesley Alaba G , César Rodríguez C , Javier Torres M , Federico Valencia L .
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Objective: We review a description of surgeries performed at the occipito- Atlanto-Axial segment in order to present our experience of the lesions diagnosed and managed at this level that required anterior decompression. An odontoidectomía was performed due to the irreducible nature of the lesion and/or because the mechanism of compression in the front, which were not susceptible to posterior approach.
Patients and methods: We report six cases in which, was used an trans oral technique to deal with the upper cervical spine segment. The cases were: four cases of rheumatoid arthritis and 2 cases of basilar impression. We described the clinical picture and the surgical technique used. Then we described the techniques used for posterior stabilization in each case.
Results: The first patient operated corresponded to a basilar impression and had dehiscence of the uvula and 1 patient (case 4) died a month after surgery due to nosocomial pneumonia and one pending fixation. The remaining patients were showed clinical improvement of symptoms and good consolidation later.
Conclusions: The trans-oral decompression surgery should be indicated in irreducible injuries and lesions where the compression is above, is recommended in other aetiologies abnormalities of bone, soft tissue or vascular. Transoral decompression - Atlanto axial instability - posterior fixation.
Clinical epidemiological characteristics of mortality of patients with intraparenchymal hemorrhage hospitalized at the Instituto Nacional de Ciencias Neurologicas
Frank Solis Ch., Jesús Félix R. , Luis Antonio T. , Rosa Ecos Q. , Carlos Abanto A.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Objective: Determine Clinical epidemiological characteristics of mortality of patients with intraparenchymal hemorrhage.
Methods: We studied patients with diagnosis of intraparenchymal hemorrhage hospitalized at the Instituto Nacional de Ciencias Neurologicas, January 2008 to December 2010. We describe the demographic and clinical variables. In addition, the logistic regression model was used to determine the factors associated with mortality in these patients.
Results: We report 129 patients, median age was 57.2 years, 56.6 % were men. We calculated a ratio of 12.4% dead; the factors significantly associated are consciousness disorder, NIHSS scale score greater than 13, and intraparenchymal hemorrhage with ventricular involvement.
Conclusions: Factors associated with mortality by intraparenchymal hemorrhage were the presence of consciousness disorder, NIHSS scale score greater than 13, and intraparenchymal hemorrhage with ventricular involvement No association was found between classical vascular risk factors, etiologic or treatment types to intraparenchymal hemorrhage mortality.
Key words: Intraparenchymal hemorrhage, mortality.