Usted está aquí
Peruvian Journal of Neurosurgery
Acute pneumocephalus in neurosurgical patients operated on in supine and prone position
ELDER CASTRO-CASTILLO.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
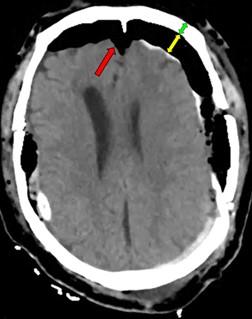
Objectives: To determine the incidence, associated factors, distribution, and degrees of acute post-surgical pneumocephalus in patients with cranioencephalic pathology operated on in the supine and prone position.
Methods: Observational, prospective, and cross-sectional study in patients 18 years of age or older, with cranioencephalic pathology belonging to the Neurosurgery Service of the Cayetano Heredia National Hospital, March 2022 - February 2023. All were operated in the supine or prone position. Acute (<= 72hrs) post-surgical pneumocephalus was identified by brain tomography. Those with pre-surgical pneumocephalus and operated on in positions other than supine and prone were excluded.
Results: Of 100 patients with cranioencephalic pathology who underwent surgery in the supine and prone position, 54% were male and 56% were under 60 years of age. In addition, 56% presented some comorbidity, and 54% had non-traumatic cranioencephalic pathology. The entire population presented some patterns of distribution and degree of postoperative acute pneumocephalus. There were no deaths from pneumocephalus. There was an association (p<0.005) between some distributions of pneumocephalus with the female sex, traumatic cranioencephalic pathology, and the creation of a surgical access to some intracranial space. In the same way, an association (p<0.005) was evidenced between the degrees of pneumocephalus of some intracranial space with the surgical opening towards this or another deeper space.
Conclusions: Acute post-surgical pneumocephalus is frequent in patients with cranioencephalic pathology operated on in supine and prone positions. The distribution and degrees of pneumocephalus may be related to sex, the type of cranioencephalic pathology, and the depth of the surgical lesion.
Keywords: Pneumocephalus, Prone Position, Intraoperative Complications, Neurosurgery. (Source: MeSH NLM)
Neurobiological basis of behavior. Is it possible to change a human being?
JASON W. RIVEROS-RUIZ
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
|
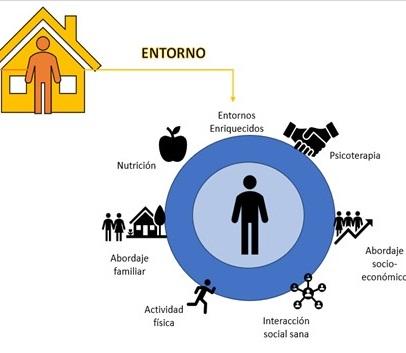
Knowledge of the neurobiological bases of behavior, and above all, mastery of the tools necessary for its modification, is essential for addressing numerous types of pathologies with clinical and social impact. Outside of the clinical setting, the prison rehabilitation system has arguably been the most neglected throughout the history of the republic in our country. Promoting innovative alternatives under the full weight of scientific evidence is a clear path to progress, thereby generating a better society, addressing the undeniable rise in the crime rate we all face every day. Shaping neurogenesis through enriched environments is a tool with promising results. People can change; we only need to change our approach to offer them even a chance for the common good of society. Keywords: Medicine, Social Change, Social Justice, Humans (source: MeSH NLM) |
Combined half and half pretemporal and subtemporal approach for petrous apex meningiomas with projection to the infratemporal fossa and petroclival region: surgical technique and outcome
LIZERT AQUINO-FABIÁN, ALLEN DIAZ I.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Introduction: Petrosal apex meningiomas are defined as tumors originating in the petrous angle and which may extend anteriorly, extending from the infratemporal region to the petroclival region. Total resection of petrous apex tumors has been considered to carry a high risk of mortality and neurological sequelae. We present the first case performed at the Hospital Nacional PNP Luis N. Sáenz using a combined pretemporal and subtemporal approach for petrous apex meningiomas projecting to the infratemporal fossa and petroclival region.
Case Report: A 55-year-old male patient with no medical history presented with a 2-year history of headache, bitemporal hemianopia, tinnitus, and paresthesias on the left side of the face. A combined half-and-half pretemporal and subtemporal approach with an infratemporal fossa projection was performed, achieving complete tumor resection and preservation of cranial nerve function, without intraoperative complications. The patient progressed favorably without a significant neurological deficit and was discharged on the 8th day.
Conclusion: The combined half-and-half pretemporal and subtemporal approach with an infratemporal fossa projection for meningiomas arising in the petrous apex with extra-axial and intradural projection and extending into the petroclival region is an effective option for the resection of highly complex tumors.
Keywords: Meningioma, Petrous Bone, Hemianopsia, Infratemporal Fossa. (Source: MeSH NLM)

Postoperative recurrence of intramedullary intraspinal Neuroenteric cyst: case report.
GUSTAVO CARLOS E., ALFONSO BASURCO C.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
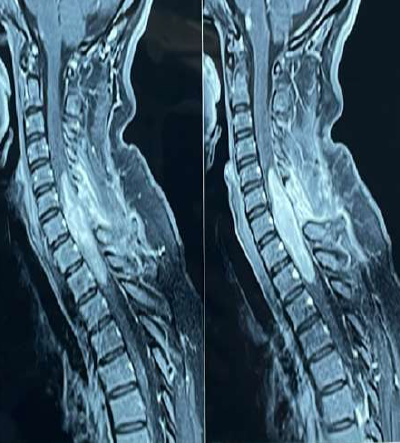
Introduction: Neuroenteric cysts (NECs) are rare, congenital, and benign lesions that result from persistent or abnormal communication between the neuroectoderm, notochord, and endoderm. They occur primarily in pediatric and young adult patients and are associated with other vertebral-medullary, gastrointestinal, and respiratory malformations. They are intradural, extramedullary lesions, with intramedullary presentation being rare. We present the case of a patient with a recurrent intramedullary intraspinal Neuroenteric cyst at the D4-D5 level.
Clinical case: A 39-year-old male patient with a history of spinal surgery for intramedullary cysts on two occasions presented with a 1-month history of moderate-intensity stabbing pain in the thoracic region radiating to the anterior region of dermatome T4, associated with predominantly left-sided paraparesis and bladder and rectal sphincter disturbances. Magnetic resonance imaging (MRI) of the cervical spine showed a hypointense cystic tumor on T1 and hyperintense on T2 at the T4-T5 level, consistent with an intramedullary Neuroenteric cyst. On examination, the patient was awake, with a Glasgow Coma Scale of 15, isochoric, photoreactive pupils, predominantly left-sided paraparesis (LLL 3/5, RLI 4/5), sensory level T5, and left patellar hyperreflexia. A T4 and T5 laminectomy was performed with evacuation of the intramedullary cyst and placement of a cysto-subarachnoid shunt, without complications. The patient's postoperative clinical course was favorable, showing recovery of motor deficits.
Conclusion: Surgical resection is the treatment of choice for Neuroenteric cysts. The goal should be total resection due to the high recurrence rate. A follow-up MRI is recommended for subtotal resections.
Keywords: Cysts, Neural Tube Defects, Neural Plate, Laminectomy. (Source: MeSH NLM)

Isolated spinal Rosai-Dorfman disease: Presentation of a recurrent case and review of literature
BRUNO A. FARIAS-VÍLCHEZ., JOSÉ FONSECA-BRICEÑO., JOSÉ NAVARRO-BARRETO.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Introduction: Rosai-Dorfman disease, also known as sinus histiocytosis, is a proliferative process characterized by painless lymphadenopathy and metabolic disorders. Central nervous system (CNS) invasion is uncommon (5%), and an isolated variant occurs in only 0.5%. Symptoms such as paresis and sensory disturbances are more frequent in the thoracic spine. Magnetic resonance imaging (MRI) is fundamental for diagnosis, which is confirmed by histopathology and immunohistochemistry studies. Surgical resection is the therapy of choice.
Clinical case: An adult female patient with no significant medical history presented with a 9-month clinical picture characterized by progressive weakness in the lower limbs. Upon examination, she was awake with left hemiparesis and preserved sensation. A cervicodorsal MRI showed an intraspinal cystic lesion within the C1-C5 spinal cord with signs of spinal cord edema and increased volume. Posterior cervical surgery with subtotal excision of the intramedullary tumor was performed. Postoperatively, the patient's clinical course was stable with quadriparesis predominantly in the lower limbs. However, in 3 months, increased paresis and sphincter disturbance were evident, leading to further surgery. Pathology and immunohistochemistry results revealed Rosai-Dorfman disease.
Conclusion: Rosai-Dorfman disease of the central nervous system (CNS) is a rare, benign disorder that can cause spinal cord invasion and spinal cord compression, resulting in paresis or sphincter disturbance. The presence of a contrast-enhancing lesion on MRI is mandatory for determining the option for surgery, and histopathological examination is essential for confirmatory diagnosis.
Keywords: Histiocytosis, Sinus, Spinal Cord Compression, Paresis, Central Nervous System (Source: MeSH NLM)
Primary amoebic meningoencephalitis due to Naegleria fowleri: case report.
GABRIEL PONCE M., ALEJANDRA VASQUEZ B., IVAN ANDÍA R., GUINEZ MUÑUICO M., ASTRID CARRIÓN C., RUBÍ ALANYA Y.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
|
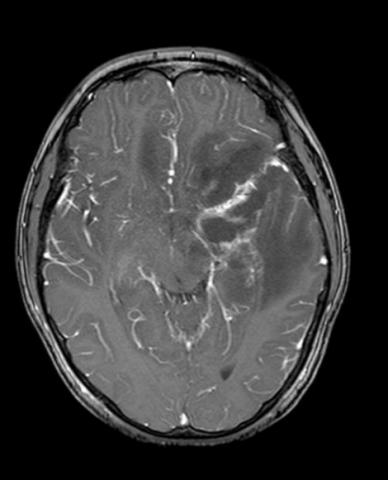
Objective: Free-living amoeba infections present with acute intracranial hypertension that are difficult to manage. In Peru, the most reported species are Balamuthia spp., Acanthamoeba spp., and Naegleria spp. We present the case of a child with a torpidly progressing amoebic meningoencephalitis, seen in our hospital in May 2023. Our objective is to describe the aggressive clinical presentation as a differential diagnosis for a brain tumor. Clinical case: A 9-year-old male patient from rural northern Peru with a history of protein malnutrition presented with an initial clinical presentation of mild headache, progressive weakness in the right side of the body, subsequently progressing to severe headache, vomiting, and neurological deterioration. Examination revealed drowsiness, global aphasia, right hemiplegia, and left ptosis. Three surgeries were performed in two stages: First, a left frontotemporal craniotomy and partial excision of a poorly defined, yellowish lesion attached to the neurovascular structures of the Sylvian valley; second, a left decompressive craniotomy and external ventricular drainage for severe intracranial hypertension. Conclusion: Treatment of cerebral amebiasis should be multidisciplinary. Early initiation of specific drugs is crucial to reduce mortality and complement surgical and intensive care treatment, given the aggressive nature of the infection. Keywords: Amebiasis, Amoeba, Naegleria, Intracranial Hypertension, Hemiplegia. (Source: MeSH NLM)
|
Endovascular treatment with coils of aneurysm of the anterior communicating artery, angiographic control, and evolution according to packing density: case series.
GABRIEL PONCE M, OSMAR ORDINOLA C, DANTE VALER G., GIANCARLO SAAL Z., JESÚS FLORES Q., RODOLFO RODRÍGUEZ V.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
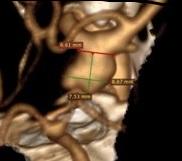
Objective: The goal of this study is to present the outcomes of endovascular treatment performed on a group of patients diagnosed with ruptured aneurysms in the anterior communicating artery. The effectiveness of the treatment will be assessed based on the degree of packing observed in both immediate and subsequent angiography control.
Methods: An observational, retrospective, and descriptive study was conducted at the Guillermo Almenara Hospital to analyze the treatment outcomes of patients with ruptured anterior communicating artery aneurysms, who were solely treated through embolization with coils (without stent or balloon) in the year 2021 and 2022. The degree of packing of the aneurysms was measured and analyzed using the AngioCalc program, while data analysis was performed using Excel.
Results: Three patients with ACom aneurysm were successfully treated using only coils for embolization. Among them, two patients had a Fisher IV subarachnoid hemorrhage (SAH) while one patient had a Fisher III SAH. The volume of the aneurysm was 12.78 mm3 for patient A, 51.65 mm3 for patient B, and 34.06 mm3 for patient C. The degree of packing of the aneurysm was calculated using a formula and found to be 23.79%, 28.7%, and 34.06% for patients A, B, and C respectively. These values were all greater than 24%. The immediate angiography results were classified as RR II for patients A and B, and RR IIIA for patient C. Subsequent angiographic control results were classified as RR IIIA for patient A, RR II for patient B, and RR IIIB for patient C. All patients had a favorable outcome.
Conclusions: The degree of coil packing affects the evolution of an embolized aneurysm, therefore serial angiographic monitoring is necessary to detect recurrence and perform additional endovascular treatment if needed.
Keywords: Aneurysm, Ruptured, Subarachnoid Hemorrhage, Angiography, Embolization, Therapeutic. (Source: MeSH NLM)
Giant unruptured posterior communicating segment aneurysm embolized in one session with stent and coils.
LIZERT AQUINO-FABIÁN, RODOLFO RODRIGUEZ V., WALTER DURAND C., DANTE VALER G., GIANCARLO SAAL Z., JESÚS FLORES Q., OSMAR ORDINOLA C.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
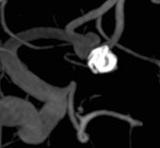
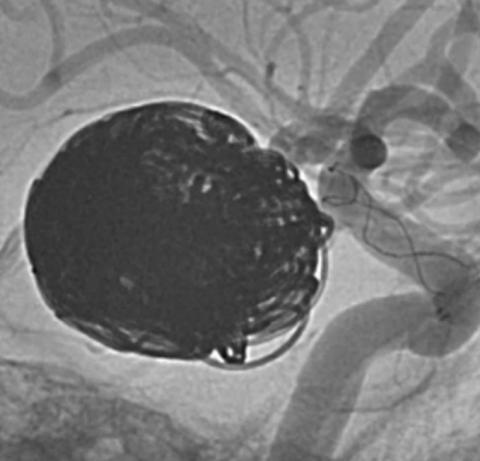
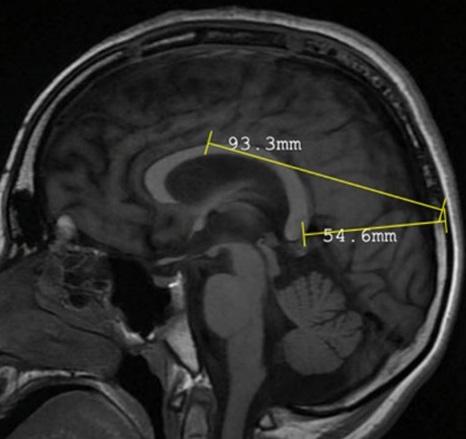
Introduction: A giant cerebral aneurysm is one that reaches a size greater than 25 mm in diameter, and whose complications are rupture and a mass effect like a tumor. The complex anatomy of the posterior communicating segment and the size of the aneurysm make it challenging to treat surgically, so the best definitive treatment option for this type of pathology is the Endovascular route, which seeks obliteration and exclusion of the aneurysm.
Clinical case: A 65-year-old female patient with a history of high blood pressure and a religion of being a Jehovah's Witness, was admitted with an illness of 5 months characterized by headache, dizziness, eyelid ptosis, left hemiparesis 4/5, on a Glasgow coma of 15 points. Cerebral angiography showed a giant unruptured aneurysm of the communicating segment of the right internal carotid artery, for which it was embolized with a stent and penumbra coils using the “Jailing” technique, successfully closing the entire aneurysm.
Conclusion: Giant aneurysms are complex lesions, for which Endovascular therapy is a safe and effective alternative with a lower complication rate.
Keywords: Intracranial Aneurysm, Cerebral Angiography, Stents, Paresis (Source: MeSH NLM)
Aneurysms and other intracranial lesions in polycystic kidney disease: illustrative case and review
ELDER CASTRO C.1, PARÍS GONZÁLEZ Q.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Introduction: Polycystic Kidney Disease (PKD) is a common hereditary kidney disease that can be accompanied by the appearance of intracranial lesions. Among these lesions, cerebral aneurysms are often found in patients with PKD, which can lead to increased morbidity and mortality. These aneurysms can have clinical and surgical implications, making them a serious concern for patients with PKD.
Clinical case: A 52-year-old man who had polycystic kidney disease in the terminal phase, untreated arterial hypertension, polycystic liver disease, and other complications related to kidney disease, was found to have two aneurysms in the anterior cerebral circulation, arachnoid cysts, and spontaneous intracranial hemorrhages. The purpose of the clinical case study and review was to understand the symptoms, risk factors, diagnosis, and management of intracranial lesions.
Conclusion: In patients with PKD, intracranial lesions like cerebral aneurysms should be suspected if there are risk factors, as they can be life-threatening if undiagnosed.
Keywords: Intracranial Aneurysm, Polycystic Kidney Diseases, Cerebrovascular Circulation (Source: MeSH NLM)
Selective posterior corpus callosotomy in a child with Lennox–Gastaut Syndrome: case report
ZINDYA BARRIENTOS M., MARCO MEJÍA T., FERNANDO PALACIOS S.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Introduction: In epilepsy refractory to medical treatment which presents multiple and bilateral epileptogenic foci such as Lennox Gastaut syndrome (LGS) the surgical alternative is disconnection surgery such as callosotomy. Posterior callosotomy is indicated in cases of atonic seizures with posterior resection, leading to better seizure control especially when resection surgeries of the anterior third or anterior two-thirds of the corpus callosum fail. We present the case of a patient with Lennox Gastaut syndrome who required a posterior callosotomy after a partial anterior callosotomy, finally achieving complete control of atonic seizures.
Clinical case: a 10-year-old male patient with a diagnosis of drug-resistant epilepsy due to Lennox Gastaut syndrome, and a surgical history of a partial callosotomy of the anterior third of the corpus callosum. In March 2021 which achieved only a transient decrease in seizures. The patient had had atonic seizures for 6 years and had been unsuccessfully treated with 5 different anticonvulsant medications such as topiramate clonazepam levetiracetam lamotrigine and valproate. On examination: Awake, alert, moderate to severe psychomotor retardation. Brain MRI was normal. A posterior microsurgical callosotomy was performed without complications. His postoperative clinical evolution was favorable showing an absence of atonic seizures.
Conclusions: Selective posterior callosotomy is an essential tool in controlling seizures in cases of refractory epilepsy in patients with atonic seizures. Our study suggests that posterior callosotomy is likely to be even more effective and safe when resections of different segments of the corpus callosum are combined.
Keywords: Corpus Callosum, Seizures, Lennox Gastaut Syndrome, Drug Resistant Epilepsy. (Source: MeSH NLM)
Central diabetes insipidus post-ventriculostomy. case report
LIZERT AQUINO-FABIÁN, ERMITAÑO BAUTISTA C.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Introduction: Diabetes insipidus is a rare complication in cerebral vascular pathology. Although its presentation is associated with surgery for pituitary tumors, few cases have been reported after the evacuation of cerebral hemorrhages.
Clinical Case: A 54-year-old male patient was admitted with a clinical picture of intense holocranial headache, Glasgow Coma Scale 8. A brain tomography (TEM) showed ventricular and basal ganglia hemorrhage. She underwent surgery, placing an external ventricular shunt, and was then transferred to the Intensive Care Unit (ICU). The control tomography showed signs of ischemia in the territory of the anterior cerebral artery. Laboratory tests showed severe hypernatremia, polyuria, hypovolemia, and alterations in urinary osmolarity, which is why she was diagnosed with central diabetes insipidus and received treatment with vasopressin, presenting a favorable evolution.
Conclusion: Central diabetes insipidus occurs due to damage to the osmoreceptors of the hypothalamus. Its incidence after brain hemorrhage evacuation surgeries is low. It is recommended to carry out exhaustive monitoring of the internal environment from the moment these patients are admitted to the Neurocritical ICU
Keywords: Diabetes Insipidus, Hypernatremia, Polyuria, Brain, Intensive Care Units. (Source: MeSH NLM)

Experience in lumbar microdiscectomy at the Guillermo Almenara Irigoyen Hospital 2018 -2021
JOHN VARGAS U., RAÚL MARTÍNEZ S., EDUARDO LAOS P., ALFONSO BASURCO C.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Objective: Herniation of the nucleus pulposus (HNP) is the leading cause of sciatica. The standard diagnostic test is magnetic resonance imaging and treatment can be conservative or surgical. The most common surgical technique is lumbar microdiscectomy. The objective of the study was to know the epidemiological and clinical profile, as well as the surgical results of patients undergoing lumbar microdiscectomy at the Almenara Hospital from January 2018 to August 2021.
Methods: Descriptive, retrospective, and cross-sectional epidemiological study. We found 82 patients who underwent lumbar microdiscectomy with complete data in the clinical history. The data was collected from the clinical history of hospitalization and outpatient consultation. Proportions were applied for qualitative variables and mean with confidence interval in quantitative variables.
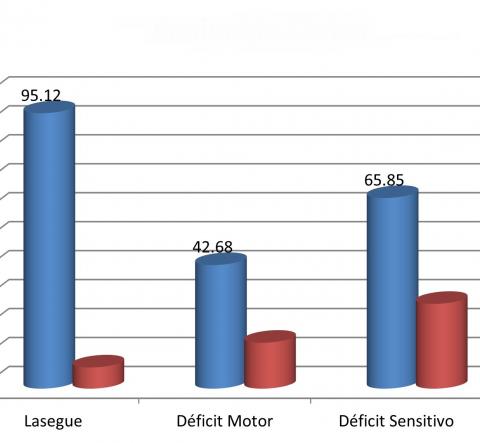
Results: Of the total number of patients, 69.51% were male, the most frequent age group was 31-50 years, and most came from Lima. The most frequently operated anatomical levels were L4 and L5. Regarding the clinic, 95.12% presented positive Lasegue. The mean preoperative VAS decreased from 7.83 to 2.00. Recurrence was 4.88% and the most frequent complication was inadvertent durotomy.
Conclusions: HNP is the most common cause of sciatica. The most frequent surgical management is lumbar microdiscectomy, which has good clinical results as well as a low rate of complications and recurrence.
Keywords: Spine, Sciatica, Nucleus Pulposus, Diskectomy, Neurosurgical Procedures. (Source: MeSH NLM)
Beginnings of endoscopy spine surgery in Peru
JERSON FLORES C.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
|
In recent years, spinal endoscopy has become increasingly common in our setting; however, its use is not recent. The first reported cases date back to the early 2010s by a team from the Cayetano Heredia Hospital in charge of Drs. Wesley Alaba and Jerson Flores. Although other minimally invasive procedures such as nucleoplasty, nucleolysis, or percutaneous rhizotomies had already been used since the 2000s, it was not until 2011 that endoscopy was used for the first time in a standardized manner in spinal surgery with the endoscope as the only element of vision, successfully resecting a vertebral lesion.
The first cases of vertebral pathology in which endoscopic surgery was used were the resection of a synovial cyst and a tuberculous abscess, followed by the resection of herniated discs at the L5-S1 level and later at the L3-L4 and L4-L5 levels. The first approach was the tubular interlaminar posterior approach, followed by the transforaminal endoscopic approach and the percutaneous posterior interlaminar approach. In the following years, endoscopy has been used not only in resecting herniated discs but also in treating central and lateral canal stenosis, reaching significant experience in this technique.
The development of spinal endoscopy and its increasingly widespread use by neurosurgeons and traumatologists from different hospitals in the country represents an important advance in spinal surgery in Peru, which brings greater benefit to patients.
Keywords: Endoscopy, Intervertebral Disc Displacement, Endoscopes, Neurosurgeons (source: MeSH NLM)
|

Spinal tuberculosis: a diagnostic challenge. case report and literature review
ZINDYA BARRIENTOS M., ALFONSO BASURCO C., ELAR CARI C., EDUARDO LAOS P.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
|
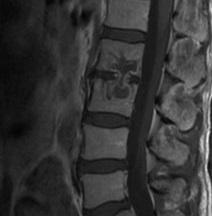
Introduction: Spinal tuberculosis TB represents 1% of all TB cases and 50 - 60 of osteoarticular TB cases.1 Certain atypical clinical and radiological presentations of spinal tuberculosis are described infrequently. 2 The lack of recognition of these presentations can lead to a delay in diagnosis and in the initiation of treatment. 3 We present the case of a patient with atypical vertebral tuberculosis operated on in our hospital.
Clinical case: A 56-year-old male with a history of diabetes mellitus no history of tuberculosis contact with a 3-year history of moderate low back pain without sciatic pain that did not improve with physical therapy The general and systemic physical examination was normal The tests showed PCR 9.8 ESR 24 BK in sputum brucellosis test and ELISA and chest X-ray were normal. A tomography and magnetic resonance imaging of the lumbosacral spine showed an osteolytic lesion involving L2 L3, isointense on T1 with regular punched-out borders sparing the L2 L3 intervertebral disc suggestive of vertebral tuberculosis He received standard tuberculosis treatment for 24 months with no improvement A new open biopsy revealed Mycobacterium tuberculosis GenXpert.
Conclusion: Spinal tuberculosis continues to be a global health problem Diagnosing atypical spinal tuberculosis remains difficult which could lead to inappropriate treatment especially regarding the choice of treatment regimens and surgical options Histopathological confirmation is essential for time management
Keywords: Tuberculosis, Spinal, Mycobacterium tuberculosis, Lumbar Vertebrae, Biopsy (Source: MeSH NLM)
|
Extrapleural transthoracic discectomy without fusion for resection of giant calcified dorsal disc hernia: case report
ANNEL MURGA V., ALFONSO BASURCO C., EDUARDO LAOS P.
Abstract (Spanish) ||
Full Text ||
PDF (Spanish)
ABSTRACT
Introduction: Calcified thoracic disc herniations are rare and their approach represents a surgical challenge when they are giant and symptomatic Surgery is indicated in cases of intractable back pain with medical management persistent intercostal neuralgia or progressive neurological deficit with the transthoracic extrapleural approach being the one of choice because it has advantages regarding the best view of the operative field We present the case of a patient with a giant calcified thoracic hernia who was successfully operated on in our hospital using an extrapleural transthoracic approach.
Clinical case: A 53-year-old male with dorsal pain in the medial region radiating to the inframammary region and progressive difficulty walking moderate proximal paraparesis T8 sensory level and urinary retention CT and MRI images showed a large calcified T6-7 disc herniation causing severe compression of the spinal cord The patient underwent a T6-7 extrapleural transthoracic discectomy plus a T6 partial corpectomy without fusion The patient tolerated the procedure well with no complications and the postoperative images one month after surgery demonstrated spinal cord decompression At follow-up irradiated back pain sensory level paraparesis and urinary retention improved.
Conclusion: Extrapleural transthoracic discectomy can be considered a safe approach in the case of giant calcified thoracic hernias since it allows resection of the calcified disc fragment and decompression of the spinal cord.
Keywords: Intervertebral Disc Displacement, Diskectomy, Spinal Cord, Decompression (Source: MeSH NLM)